The Sacrum Paradox: Keystone or Suspension?

Why It Matters: The Sacroiliac Joint
For proper treatment of our body’s structural core, the sacroiliac joint, it is important that we understand how it functions properly. Misconceptions regarding the interrelationship of ligaments and muscles, the shape and movement pattern of the sacroiliac joint, and other factors disguise many complications and contraindications that make treatment challenging.
 Is The Sacrum a Keystone or is it Suspended?
Is The Sacrum a Keystone or is it Suspended?
Whether the sacrum functions as a keystone or is suspended from the ilia has been debated for well over one hundred years. In the early 1990s Vleeming and Stoeckart[1] and, separately, Snijders[2], published their findings that the sacrum fits into a receptacle, like a keystone in a Roman Arch. On the other hand, DeJarnette states that the sacrum does not touch the ilia.
Vleeming’s Perspective
Vleeming stated “the bone (sacrum) is wider cranially than caudally and wider anteriorly than posteriorly. Such a configuration permits the sacrum to become ‘wedged’ cranially and dorsally into the ilia within the pelvic ring.”
DeJarnette’s Perspective
DeJarnette[3] stated “The sacrum is wedge-shape from above downward, its base articulating with the fifth lumbar vertebra; it is also wedge-shaped from backward, a fact that makes clear the statement that the sacrum is held suspended between the innominates by strong ligaments instead of completing the bony girdle as the keystone caps the arch.”
The question that arises is how can both authors give the same description of the sacrum and its physical relationship to the ilia and come to opposite conclusions of their function? Is the sacrum a keystone or is it suspended?
Force Transfer Between Sacrum and Ilia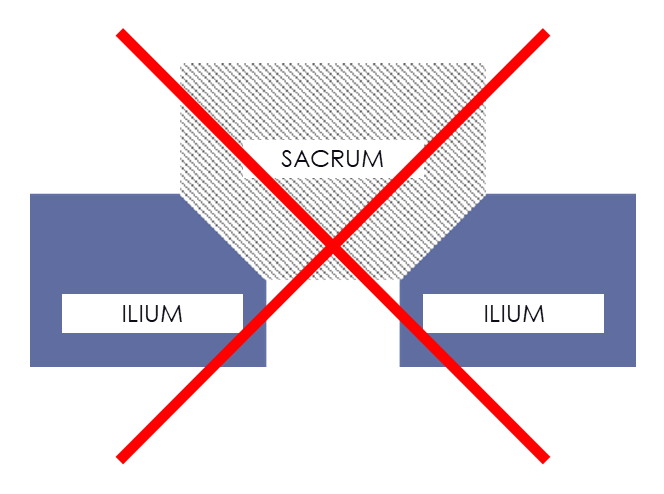
The main difference between the two concepts of a keystone and a suspension system is how force transfers between the sacrum and ilia.
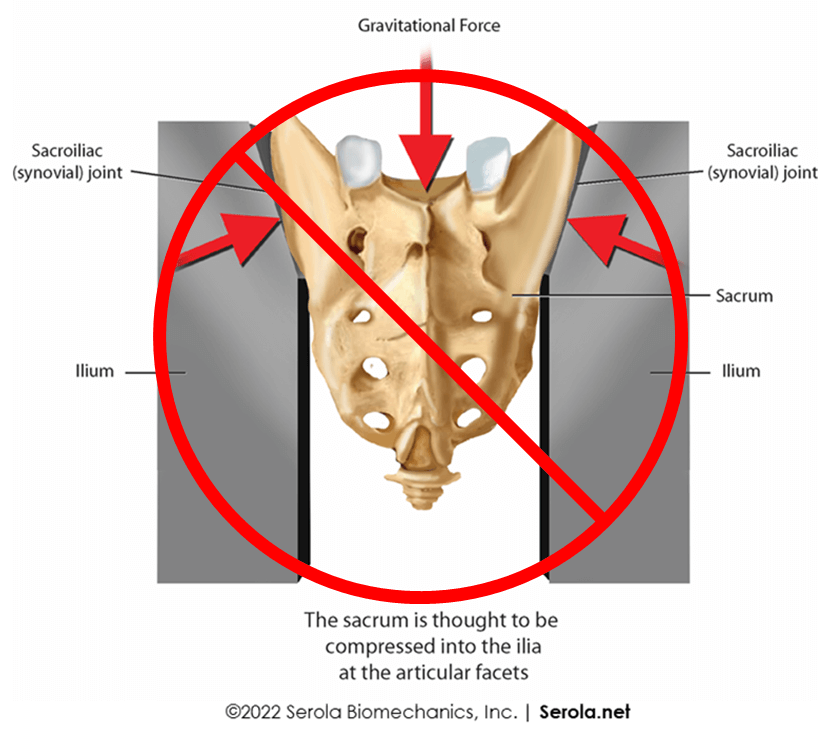
Vleeming, et al.[1] proposed that at the end of range of motion, the sacrum is upright and the sacral and iliac articular surfaces would be compressed together. Supposedly, the vertical placement of the sacrum positions the facets to slide inferiorly into the receptacle formed by the ilia, as in a keystone, and contributes to its stability within the pelvic ring.
In other words, when he initially described form and force closure as components of the keystone concept, he defined counternutation, in which the sacrum is more vertical, as being the position of stability during force transfer. The dorsocranial “wedging” of the sacrum into the ilia occurs at the end of range of motion in counternutation where “bone contact force” prevents further movement of the sacrum inferiorly as well as posteriorly (dorsally). If this were true, the ligaments would not play a role in stabilization during weight transfer because the bones would be performing that function.
Paradoxically, he more recently continued to advocate dorsocranial wedging as a key component of form closure, but also recognized that “in self-bracing of the pelvis, nutation of the sacrum is crucial”[10], in which the sacrum is more horizontal. The contradiction is evident, if not immediately recognized.
 Further, claiming that the SIJ articular surfaces are flat, Snijders[2] drew force vectors that supposedly intersected at the SIJ to provide a “self-bracing effect” of a flat SIJ. Although he briefly mentioned that the SIJ surfaces were propeller shaped, he attributes that to counteracting flexion and then ignores the actual shape of the facets and continues as if they were flat.
Further, claiming that the SIJ articular surfaces are flat, Snijders[2] drew force vectors that supposedly intersected at the SIJ to provide a “self-bracing effect” of a flat SIJ. Although he briefly mentioned that the SIJ surfaces were propeller shaped, he attributes that to counteracting flexion and then ignores the actual shape of the facets and continues as if they were flat.
Conversely, a suspended sacrum transfers force through the syndesmosis by the ligaments, more like a hammock. Instead of force pushing one bone into the other, placing the weight of the entire upper body at two relatively small points, the force pulls one bone towards the other through a mass of ligaments with contact points spread throughout the sacrum: in this manner, force transfers from bones to ligaments to bones to ligaments etc.
The large mass of pelvic ligaments is part of a system that directly or indirectly connects every bone in the body to every other bone. Their relative positions and movements are self-regulated via proprioceptive reflexes, using the muscles to ensure maximum stability by adapting to external forces or injury. As such, every bone, ligament, and muscle are parts of a tensegrity system where stability is shared by the entire kinematic chain.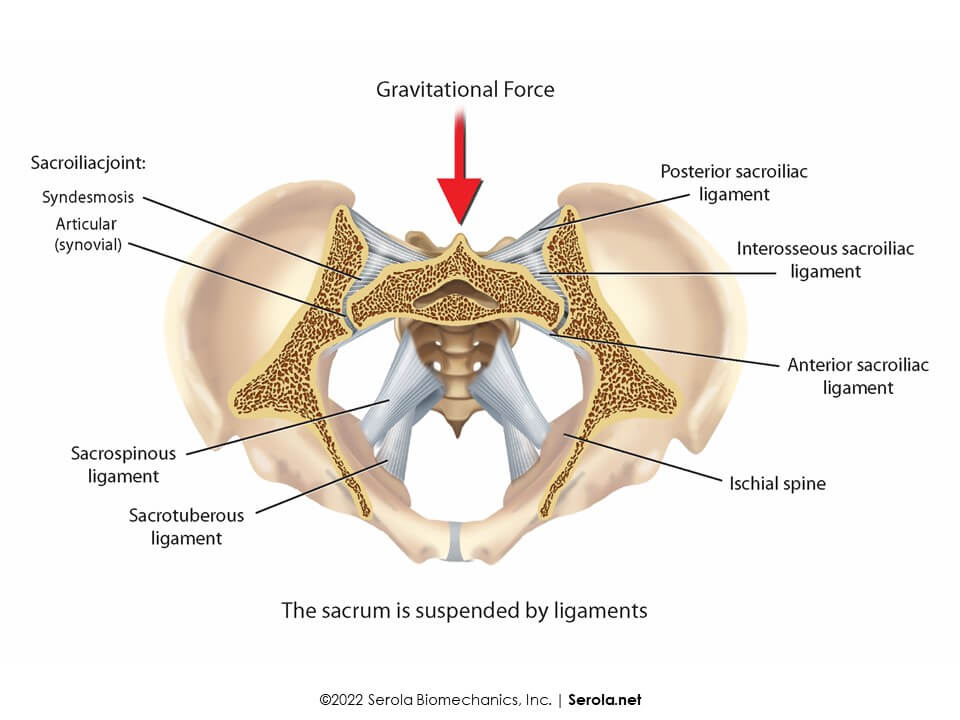
In accordance with De Jarnette, it should be noted that, during nutation, the wider anterior-narrower posterior shape of the sacral base demonstrates a requirement for the sacrum to drop anteriorly and inferiorly away from the ilia during weight bearing, into a more horizontal position. Since the sacrum is below the ilia in the horizontal position, the anatomical function of the large mass of ligaments in suspending the sacrum from the ilia becomes evident.
The Ligament & Muscle Complex: Two Factors in Joint Stability
It is well known that ligaments are the primary stabilizers of a joint. When the ligaments sprain, the muscles act as secondary stabilizers. Let’s take a closer look at that relationship with regard to the sacroiliac joint.
Unfortunately, many health care professionals consider the sacrum to be a keystone and promote stretching without regard to the ligaments that stabilize the joint. Because tight muscles are painful due to hypoxia, stretching increases blood flow and the resulting oxygenation relieves pain, so it appears that the condition is healed, but is it? And does that affect the ligaments, and if so, how?
The Treatment Paradox
Since nutation is the most stable position of the normal SIJ, strengthening and stretching programs are designed to promote nutation, but without consideration to the idea that the ligaments limiting nutation are torn.
If the sacrum is a keystone, stretching shouldn’t affect it. But if the sacrum is suspended by ligaments, when sprained, the stretched nutation limiting ligaments would generate a ligamento-muscular reflex that causes the counternutation muscles to tighten to limit nutation.
If not for the counternutation muscles, the sacroiliac joint can easily be forced past normal range of motion, into excess nutation, and further damage the ligaments. As a result, the muscles will re-tighten to protect the ligaments, forming a positive feedback loop: torn ligaments → tight muscles → stretch muscles/ligaments → more torn ligaments → more muscle tightening, etc. It is not always easy to make the association because, in some cases, the muscles may take days to re-tighten and become painful. How do we resolve this contradiction?
The key to proper treatment is to stabilize the joint externally by a compressive force, such as a brace or belt, and then stretch the muscles; in this manner, stretching is relatively safe and effective. Be careful not to overpower the muscles with too strong a force. If the joint is properly stabilized and excessive force is not used, strengthening and stretching can be very beneficial.
Scientific Studies – Keystone vs. Suspension
There are no scientific studies that demonstrate that the sacrum acts as a keystone, or that weight bearing goes through the articular facets.
Conversely, Cusi [11] stated that load transfers through the posterior sacroiliac ligaments, including the interosseous sacroiliac ligaments.
To further support ligamentous suspension, Vukicevic et al. [12], using holographic analysis, applied a wide range of loads to 12 cadaveric pelves with preserved lumbar spines, hip joints, and ligaments. They found that “tight contact between the articular surfaces is never reached in a wide range of the applied loads, secured by strong sacroiliac interosseous ligaments.”
Conclusion: Form & Function
Keystone proponent’s claim that both counternutation and nutation are necessary positions of stability for force transfer through the sacroiliac joint are contradictory statements.
Since forces occurring during load transfer force the sacrum anteriorly and inferiorly into nutation, there is no practical need for the sacrum to be ‘wedged’ dorsally. To speak of wedging the sacrum dorsally is misleading and only serves as a distraction from considering true anatomical form and function.
While the weight of the upper body drives the sacrum into nutation, no mechanism of force transfer has been explained that drives the sacrum into counternutation, during which the sacrum supposedly shifts to a vertical position.
De Jarnette’s description of sacral suspension is consistent and makes biomechanical sense. Stability is needed during nutation when the weight of the entire upper body is held by the sacrum and transferred to the ligaments, where force is absorbed, and range of motion is regulated.
Proper sacroiliac joint treatment involves externally stabilizing the joint during strengthening or stretching programs.
References:
- Vleeming, A. and R. Stoeckart, The role of the pelvic girdle in coupling the spine and the legs: a clinical-anatomical perspective on pelvic stability, in Movement, Stability, & Lumbopelvic Pain, A. Vleeming, D. Mooney, and R. Stoeckart, Editors. 2007, Churchill Livingstone Elsevier. p. 229-237.
- Snijders, C.J., Transfer of Lumbosacral Load to Iliac Bones and Legs: Part 1 – Biomechanics of Self-Bracing of the Sacroiliac Joints and its Significance for Treatment and Exercise. Clinical Biomechanics, 1993a. 8: p. 285-294.
- De vJarnette, M., Sacro Iliac Technic. 1938: Self Published.
- Vleeming, A., et al., The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. J Anat, 2012. 221(6): p. 537-67.
- Solonen, K.A., The sacroiliac joint in the light of anatomical, roentgenological and clinical studies – 127 pages. Acta Orthop Scand Suppl, 1957. 27: p. 1-127.
- DonTigny, R.L., Function and pathomechanics of the sacroiliac joint. A review. Physical Therapy, 1985. 65(1): p. 35-44.
- Snijders, C.J., Transfer of Lumbosacral Load to Iliac Bones and Legs: Part 2 – Loading of the Sacroiliac Joints when Lifting in a Stooped Position. Clinical Biomechanics, 1993b. 8: p. 295-301.
- Levin, S.M., The Sacrum in Three-Dimensional Space. Spine: State of the Art Reviews, 1995. 9(2): p. 381-88.
- Moore, K.L., A.F. Dalley, and A.M. Agur, Clinically Oriented Anatomy. 6th Edition ed. 2010, Baltimore, MD: Wolters Kluwer / Lippincott Williams & Wilkins.
- Vleeming, A. and M. Schuenke, Form and Force Closure of the Sacroiliac Joints. PM R, 2019. 11 Suppl 1: p. S24-S31.
- Cusi, M. SPECT-CT on patients with a clinical diagnosis of failure of load transfer of the sacro-iliac joint. in 7th Interdisciplinary World Congress on Low Back & Pelvic Pain. 2010. Los Angeles: 7th Interdisciplinary World Congress on Low Back & Pelvic Pain.
- Vukicevic, S., et al., Holographic analysis of the human pelvis. Spine, 1991. 16(2): p. 209-14.
