
Multifidus
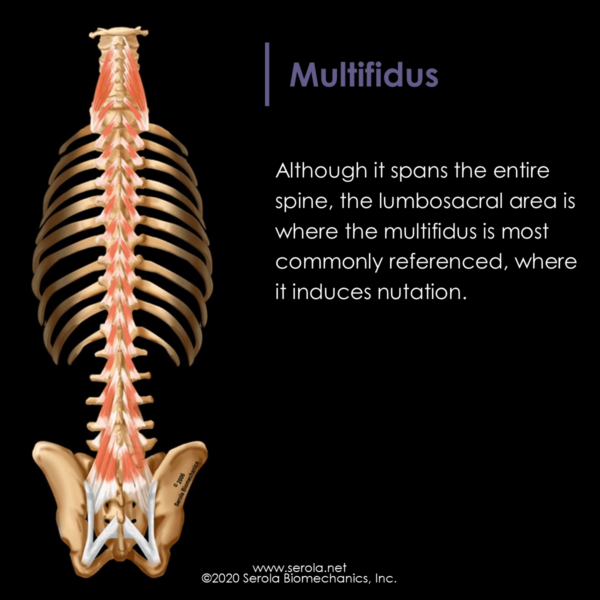
Although it spans the entire spine, the lumbosacral area is where the multifidus is most commonly referenced, where it induces nutation.
Origin: spinous processes of vertebrae C2-L5
Insertion: transverse process of vertebrae 1-4 levels below, including the sacrum, and to the erector spinae aponeurosis. Some fibers from L1-2-3 insert at the posterior superior iliac spine.
Functions:
- Provides fine control of vertebral movement.
- C-5 to L3: Causes nutation by flattening the thoracic curve
- L3-Sacrum: Causes nutation by increasing lordosis and helping prevent flexion induced by the oblique abdominals [1]p103
- L1-2-3 to PSIS: These fibers may cause counternutation by pulling the ilia superiorly – more study is needed.
The multifidus can be palpated just medial to the PSIS. It is the largest muscle spanning the lumbosacral area. It joins with the gluteus maximus and superficial erector spinae to form a connective tissue sheath, the gluteus raphe, which connects these three very powerful back muscles into one extensor (nutation) unit spanning the lumbar spine, pelvis, and hip.
Wilke [2] showed that the multifidus has the strongest influence, of all back muscles, on lumbar segmental stability. Consequently, inhibition, as seen in the nutation lesion, can adversely affect lumbar stability.
Since the multifidus spans the entire spine, it is important to be more specific as to the level of injury. With this in mind, it should be noted that Hides [3-5]p70-76 found cross-sectional asymmetry at the L4/L5 and L5/S1levels in patients with low back pain. The symptomatic side was found to be significantly smaller, exhibiting wasting of the tissues, even within 24 hours after injury. However, no differences were found at the upper lumbar levels between subjects with low back pain and normal subjects. And, asymptomatic individuals had relatively symmetrical multifidus sizes at all levels. Hides et al. suggested that reflex inhibition of the specific multifidus was likely. This pattern is what we would expect with a nutation lesion because, at those levels, the multifidus would provide a strong nutation moment and aggravate the nutation lesion; therefore it would be inhibited.
Another study by Alaranta et al.[6] also found that the paraspinal muscles at L3 to S1 showed fatty degeneration at the level of the lumbosacral area, but not at the upper lumbar levels, in people with self-reported chronic low back pain. They stated that their study indicated that L3 to S1 is the area that should be looked at in low back pain. Fatty degeneration indicates that the tissue is not receiving adequate neural input due to inhibition, which is what we would expect in the nutation lesion. On the other hand, the lumbar vertebrae above L3 did not show any fatty degeneration, which indicates that, because they may be involved in counternutation, they were not inhibited.
Deandrade [7] stated “There is some association between reflex muscle inhibition and the muscle atrophy that is seen in patients with joint disease. However, neurogenic muscle atrophy results only from a lower motor neuron. On the other hand, disuse atrophy is due to a functional lack of excitation of the motoneuron supplying the muscles. A depression of excitation has been demonstrated to result from reflex inhibition due to joint distension and other stimuli.” In the nutation lesion, we see reflex inhibition of nutation pattern muscles.
References:
- Bogduk, N., Clinical Anatomy of the Lumbar Spine and Sacrum. 2005: Elsevier Churchill Livingstone.
- Wilke, H.J., et al., Stability increase of the lumbar spine with different muscle groups. A biomechanical in vitro study. Spine, 1995. 20(2): p. 192-8.
- Hides, J., et al., Multifidus size and symmetry among chronic LBP and healthy asymptomatic subjects. Manual Therapy, 2006.
- Hides, J.A., C.A. Richardson, and G.A. Jull, Multifidus muscle recovery is not automatic after resolution of acute, first-episode low back pain. Spine, 1996. 21(23): p. 2763-9.
- Richardson, C., et al., Therapeutic Exercise for Spinal Segmental Stabilization in Low Back Pain. 1999: Churchill Livingstone.
- Alaranta, H., et al., Fat content of lumbar extensor muscles and low back disability: a radiographic and clinical comparison. Journal of Spinal Disorders, 1993. 6(2): p. 137-40.
- Deandrade, J.R., C. Grant, and A.S. Dixon, Joint Distension and Reflex Muscle Inhibition in the Knee. The Journal of Bone and Joint Surgery. American volume, 1965. 47: p. 313-22.