
Front & Back Muscle Slings
This article is actually a combination of two other muscle slings, the Internal – External Obliques and Gluteus Maximus – Latissimus Dorsi. I present them in one article to show how they function together to create the same exact movements at the sacroiliac joints.
Coordinated Rotation of the trunk
In normal movement, during weightbearing on the right foot (stance phase – right nutation -pelvis rotating to the right) the left internal oblique and right external oblique rotate the shoulders to the left, while the left latissimus dorsi (LD) and right gluteus maximus (GM) simultaneously rotate the shoulders to the left, causing left lumbar rotation coupled with left lateral flexion. This coordinated movement results in nutation on the right and counternutation on the left and is consistent with Gracovetsky’s [1] analysis of muscular patterns in shoulder counterrotation during gait. Normally, these patterns reverse during gait when weight bearing switches to the left side.
Gracovetsky found that when the right leg is in extension (stance phase – right nutation – pelvis rotating to the right), the right shoulder would rotate to the left and the muscle patterns are:
-Contracted left: trapezius, posterior deltoid, latissimus dorsi.
-Inhibited left: gluteus maximus, pectoralis major, anterior deltoid, anterior serratus.
-Contracted right: gluteus maximus, pectoralis major, anterior deltoid, anterior serratus.
-Inhibited right: trapezius posterior deltoid and latissimus dorsi.
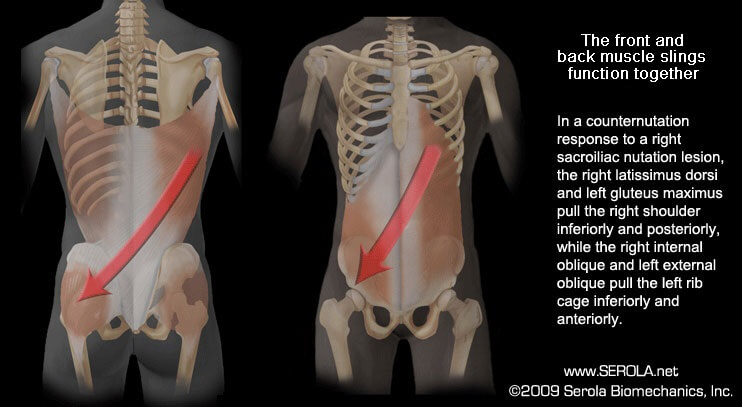
In coordination with the above pattern, the right internal oblique and left external oblique pull the left rib cage inferiorly and anteriorly, while the right latissimus dorsi and left gluteus maximus pull the right shoulder inferiorly and posteriorly, simultaneously causing right rotation coupled with right lateral flexion (counternutation).
Sacroiliac Nutation Lesion
The difference that the sacroiliac nutation lesion presents from normal movement is mainly that the sprained ligaments on the right activate a reflex to induce and sustain a counternutation pattern in order to keep stress off the SIJ ligaments. A nutation lesion would activate muscular responses that maintain a state of counternutation on the side of injury, in this case the right side.
In a right nutation lesion, the actions of the muscles inducing counternutation on the right become intensified while those of the muscles inducing nutation on the right become inhibited; thus, the left GM and right LD will tighten, and the right GM and left LD will be inhibited. This force couple induces nutation on the left, as demonstrated by decreasing tension in the left long dorsal sacroiliac ligament [2]. At the same time, it would induce counternutation on the right.
With chronicity, as evident in a nutation lesion, the muscles that induce counternutation on the side of injury remain in a state of tension throughout both nutation and counternutation. The worse the injury, the stronger the muscular reaction, and the greater tendency for the body to remain in counternutation on the side of injury, even during stance phase. Over time, this pattern may lead to structural distortions and coordination difficulties that may be expressed by delayed timing and reduced balance and performance throughout the body.
Reference:
1. Gracovetsky, S. and H. Farfan, The optimum spine. Spine, 1984. 11(6): p. 543-73.
2. Vleeming, A., et al., The function of the long dorsal sacroiliac ligament: its implication for understanding low back pain. Spine, 1996. 21(5): p. 556-62.