
Muscular Adaptations Overview
Historical Perspective / A New Model
Until relatively recently, the sacroiliac joint was considered fused and immobile. Now, even though the sacroiliac joint has been proven to be mobile, the misconception persists that, since very few muscle strands actually cross the sacroiliac joint, it is not moved by muscles. Instead, it is mistakenly thought to be moved solely by the mass of the trunk acting upon the pelvis in various postures [1-3]. Contrary to these conventional concepts, Dr. Serola’s Musculoskeletal Integration Theory demonstrates that the sacroiliac joint is not only moved by muscles, but that the muscles that attach to the innominates and/or sacrum play a key role in integrating the entire musculoskeletal system through nutation and counternutation patterns, in which the sacroiliac joint is the core structure.
Muscular Response to SIJ Injury
Hilton’s Law states that, in any joint, “The same trunks of nerves whose branches supply the groups of muscles moving a joint, furnish also a distribution of nerves to the skin over the insertion of the same muscles, and the interior of the joint receives its nerves from the same source.” With this law, he stressed the interdependence of the articular structures, e.g. ligaments, muscles that move the joint, and the overlying skin. In agreement with Hilton’s Law, it can be said that, in any joint, the muscles that attach to the bones that comprise the joint are regulated by the ligaments within the joint by sharing the same nerve pathways.
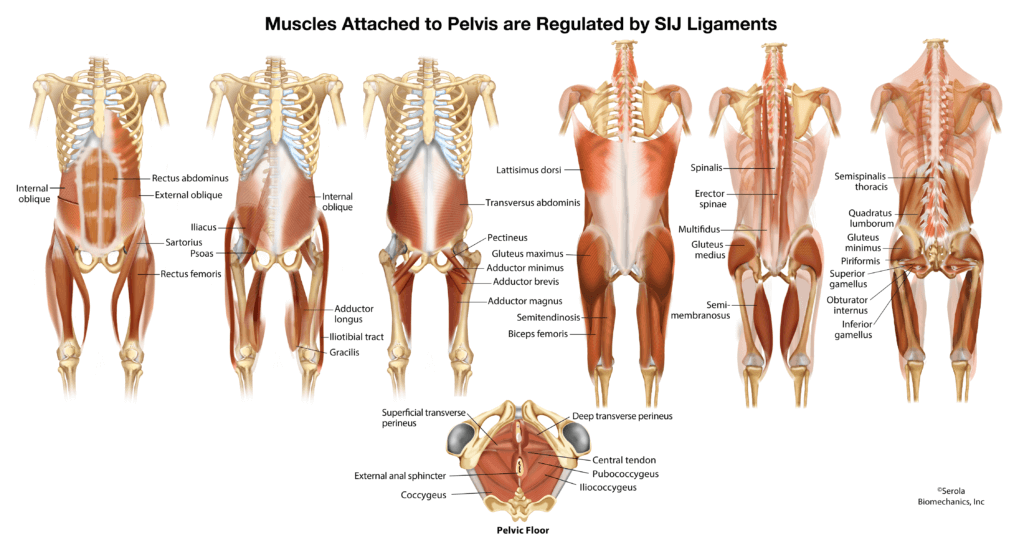
With the realization that almost every muscle from the head to the knees directly attaches to the sacrum or innominates (see figure), it is readily apparent that the greatest bulk of our musculoskeletal system is directly regulated by the sacroiliac joint. With this perspective, it should be apparent that injury to the sacroiliac ligaments must generate a significant effect on the entire musculoskeletal system.
The Musculoskeletal Integration Theory proposes that sacroiliac joint movement occurs through forces generated by the muscles that attach to the sacrum and/or innominates, acting through a combination of vectors dependent on their attachment points and angles of pull, in accordance with the alignment of the synovial (articular) region of the joint.
Positioned at the center of shock absorption, the sacroiliac joint functions as a regulator of pelvic and trunk muscles and thereby influences posture and lumbar segmental stability [4-6]. In its healthy state, the weight-bearing region of the sacroiliac joint is supported by balanced muscular action which ensures smoothly coordinated movement.
However, upon injury to the ligamentous system, structural stabilization is transferred to secondary systems. Muscular coordination is compromised for joint stability. Ligament laxity allows increased separation of the sacral surface from the iliac surface and weight bearing becomes compromised. The structural framework shifts to distribute gravitational and muscular forces in a manner that avoids overloading the injured joint.
Although, in the literature, far more attention is given to the articular area’s role in motion and dysfunction, the Musculoskeletal Integration Theory suggests that the most significant dysfunction develops though lesion of the posterior ligamentous weight-bearing system. While muscle splinting patterns occur principally for stabilization of the compromised weight-bearing system, the movement patterns they generate are in line with the configuration of the synovial region of the joint.
Muscle Classifications
The Musculoskeletal Integration Theory divides the muscles into two groups, nutators and counternutators, which reciprocate during movement. Nutators are most active during weight bearing, driving the sacroiliac joint toward the bottom point of shock absorption. Counternutators become most active at the bottom point of shock absorption, to lift the sacrum and ilium into rebound (see Shock Absorption).
Nutators on one side will facilitate counternutation on the contralateral side, and vice versus.
Side of Injury
When the lesion is nutation, the muscles respond in a manner to avoid placing stress on the nutation limiting ligaments by activating the counternutators and inhibiting the nutators on the side of injury.
Side of Non-Injury
On the contralateral side, due to the reciprocating pattern of movement, the opposite reaction occurs; activating the nutators and inhibiting the counternutators (see Ligamento-muscular Reflex).
Maintenance of Joint Tension
In terms of contraction/inhibition, nothing is absolute; there is no “on” or “off.” The body moves in relative phases. When the nutators are active, the ipsilateral counternutators are relatively inhibited, and vice versus. In other words, while the “active” muscles are concentrically contracting (shortening), the “inhibited” muscles are eccentrically contracting (lengthening). At the bottom point of shock absorption, ligaments absorb the load, and the concentric/eccentric correlation switches; in this manner, tension is maintained within the musculoskeletal system (see Muscle-Ligament Role in Joint Tension).
Systemic Effects
In agreement with Johansson and Sojka’s hypothesis [7], Bullock-Saxton [8], Phillips [9], and Solomonow [10, 11] demonstrated that both sensory and motor changes are evident in muscles distant to the bones comprising an injured joint. Bullock-Saxton suggested that “…the arthrokinetic reflex might be considered as a triggering factor that would initiate a whole chain of adaptation reactions, eventually resulting in changed movement patterns” … as proposed by Lewit [12]p13 and Janda {Janda, 1978 #1235], which are not limited to the side of injury, but could influence the uninjured side. She continued saying “Because muscles respond in different ways to peripheral injury, the results of this study suggest that the effects need to be sought in areas remote from the site of injury.”
With new insight into the relationship between the SIJ and the muscles that move it, as expressed in the Musculoskeletal Integration Theory, the concepts in the above paragraph are explained more simply. The other end of every muscle that attaches to the pelvis also attaches to another structure in the trunk, pelvis, or extremities. It follows that injury to the sacroiliac ligaments would indirectly affect distant joints in a cascading effect throughout the musculoskeletal system.
Depending on the degree of injury, and the length of time in compensation, the muscles will alter the structure, initially causing a twist to the spine and pelvis, which will eventually manifest as dysfunctions anywhere in the musculoskeletal system (see Overcompensation Pattern – Structural Adaptations, Spinal – Pelvic Syndromes, and Associated Conditions), depending on use and other factors (see Chronicity Factors).
References:
- Solonen, K.A., The sacroiliac joint in the light of anatomical, roentgenological and clinical studies. Acta Orthopaedica Scandinavica. Supplementum, 1957. 27(Suppl 27): p. 1-127.
- Mitchell, F.L., Jr. and P.K.G. Mitchell, The Muscle Energy Manual. Vol. 3. 1999, East Lansing: MET Press.
- Bogduk, N., Clinical Anatomy of the Lumbar Spine and Sacrum. 2005: Elsevier Churchill Livingstone.
- Snijders, C.J., Transfer of Lumbosacral Load to Iliac Bones and Legs: Part 1 – Biomechanics of Self-Bracing of the Sacroiliac Joints and its Significance for Treatment and Exercise. Clinical Biomechanics, 1993a. 8: p. 285-294.
- Indahl, A., et al., Sacroiliac joint involvement in activation of the porcine spinal and gluteal musculature. Journal of Spinal Disorders, 1999. 12(4): p. 325-30.
- Marshall, P. and B. Murphy, The effect of sacroiliac joint manipulation on feed-forward activation times of the deep abdominal musculature. Journal of Manipulative and Physiological Therapeutics, 2006. 29(3): p. 196-202.
- Johansson, H. and P. Sojka, Pathophysiological mechanisms involved in genesis and spread of muscular tension in occupational muscle pain and in chronic musculoskeletal pain syndromes: a hypothesis. Med Hypotheses, 1991. 35(3): p. 196-203.
- Bullock-Saxton, J.E., Local sensation changes and altered hip muscle function following severe ankle sprain. Physical Therapy, 1994. 74(1): p. 17-28; discussion 28-31.
- Phillips, D., et al., Ligamentomuscular protective reflex in the elbow. The Journal of Hand Surgery. American volume., 1997. 22(3): p. 473-8.
- Solomonow, M. and M. Krogsgaard, Sensorimotor control of knee stability. A review. Scandinavian Journal of Medicine & Science in Sports, 2001. 11(2): p. 64-80.
- Solomonow, M., Ligaments: a source of work-related musculoskeletal disorders. Journal of Electromyography and Kinesiology, 2004. 14(1): p. 49-60.
- Lewit, K., Manipulative Therapy in Rehabilitation of the Locomotor System. 2nd ed. 1991, Oxford: Butterworth-Heinemann.